{kind=link}
Here's something you might be interested in.
Ask a Hipster — Advice you didn't know you needed
Big Screen — Movie commentary
Blurt — Music's inside track
Booze News — San Diego spirits
Classical Music — Immortal beauty
Classifieds — Free and easy
Close to Home — What it’s like on the street where you live
Cover Stories — Front-page features
Drinks All Around — Bartenders' drink recipes
Excerpts — Literary and spiritual excerpts
Feast! — Food & drink reviews
Feature Stories — Local news & stories
Fishing Report — What’s getting hooked from ship and shore
From the Archives — Spotlight on the past
Golden Dreams — Talk of the town
The Gonzo Report — Making the musical scene, or at least reporting from it
Letters — Our inbox
Movies@Home — Local movie buffs share favorites
Movie Reviews — Our critics' picks and pans
Musician Interviews — Up close with local artists
Neighborhood News from Stringers — Hyperlocal news
News Ticker — News & politics
Obermeyer — San Diego politics illustrated
Outdoors — Weekly changes in flora and fauna
Overheard in San Diego — Eavesdropping illustrated
Poetry — The old and the new
Reader Travel — Travel section built by travelers
Reading — The hunt for intellectuals
Roam-O-Rama — SoCal's best hiking/biking trails
San Diego Beer — Inside San Diego suds
SD on the QT — Almost factual news
Sheep and Goats — Places of worship
Special Issues — The best of
Street Style — San Diego streets have style
Surf Diego — Real stories from those braving the waves
Theater — On stage in San Diego this week
Tin Fork — Silver spoon alternative
Under the Radar — Matt Potter's undercover work
Unforgettable — Long-ago San Diego
Unreal Estate — San Diego's priciest pads
Your Week — Daily event picks
University Hospital's ER takes 'em all
Life, death, and in between
The police officer pushes his prisoner, locked in a wheelchair, through the Emergency Room doors. The man, a well-dressed scuffler, sits with his head on his chest and says nothing as the officer checks in at the front desk. The
officer then wheels the chair through Emergency Surgery and into an examination room in Emergency Medicine, where he locks the man to his bed.
“We caught him inside a department store where we’ve had around $125,000 in burglaries lately,” the officer says. “His modus operandi fits the pattern. The burglar hides in the store just before closing, under a bed or something, then when everybody’s gone, he’ll get up, get the stuff he wants, no more than he can run with, throw a chair through a window, and break out. It takes us a few minutes to get there, wherever we are, so he might get away. But this guy set off a silent alarm in the fur locker.”
The prisoner’s chains rattle and the officer ducks into the room.“I want to take off my coat,” the man says.
The officer unlocks the cuffs and, stiff-armed, helps the prisoner with his coat, keeping one hand at his gun-side. When the coat is off, he locks the man to his bed again.
“What did you bring him to the ER for?” the nurse asks.
“Says he’s sick. Says he passed out and just woke up. He called our dispatcher about the same time we were pulling into the parking lot and said he was locked in the store. I don’t know if he’s the one we’ve been looking for. But the fur locker’s one floor down and the other side of the building from where he says he passed out. He’s got a record, too. How does he look to you?” he asked the nurse.
She shrugs.“Most of the ones you bring in are frauds. ‘Chest pains’ and ‘fainting.’ I know you’re obligated by law to bring the guy here if he says he’s sick. Oh, well, it buys him some time, and he gets a free checkup. Besides,” she adds, “we might find something.”
The Emergency Room at University Hospital greets its patients with the neutrality of a business office. They walk or roll or are carried through its pneumatic glass doors into the familiar atmosphere of nothing special: forms to sign and phones and IBM cash registers going tacka-tack. The doctors are rarely dressed in surgical white; they wear, instead, striped shirts, bow ties, Wallabees. The centrifuge in the back room, with its little vials of blood spinning out and around, whirs constantly, but it could as easily be the sound of a vacuum cleaner or Star Trek on a faraway television, and the sound blends easily with the hum of small talk.
The walls are white. Not a clinical white, but working white, trimmed with hard, bright red, violet, and orange at the doors and counters.
If you were to wake up here, staring at the tiny holes in the ceiling tile and wondering where you were, you might simply think you were in a freshly painted room. You’d probably never guess that the only hint of a smell was wet cast plaster.
You might think you hadn’t been noticed. But someone sees you from the corner of their eye and asks if there’s anything they can do.
The ambulance radio announces a fight victim coming in. Two minutes later the victim rolls through the door, his jean jacket and clothing stuffed on the rack below the gurney. Except for his eyes, which he opens and closes slowly, halfway, he doesn’t move. His friend, in jeans and jacket, with a wine bota slung over his shoulder, walks alongside.“You’re going to be okay, man. You just take it easy, okay?” The man on the gurney, already being wheeled into the emergency surgery exam room, doesn’t answer.
Nurses help the man onto an examination table. A pulpy blue wound covers his forehead and he moves his body sluggishly. While they inventory his personal belongings, nurses and staff try to coax his name, his cooperation, any response from him. He doesn’t talk, only opens and closes his eyes.
When the doctor comes, he asks the man what has happened. The man moves his lips, but no sound comes out. “Have you been taking any drugs?” the doctor asks, then turns to the man’s friend, watching from the doorway. “Has he done any drugs tonight?”
“Just a couple of brews. Maybe a quart...”
The doctor turns back to the table.“Put your tongue out. Okay, now show me all your teeth.”
The friend walks around to the head of the exam table. “Say something, man.” No answer. “Hey, is he going to be all right?”
“What happened to him?” the doctor asks.
“These guys jumped him in Horton Plaza. Two big guys, man, for no reason. I can’t believe this — he’s a healthy dude.”
The doctor returns to his patient.“Can you lift your feet? Good. It’s important that you answer the questions, all right?” The doctor presses his fingers around the forehead wound. “This hurt? This?” Suddenly the man lurches upright, shouting, “Hey, man, hey, man,” groping in the air.
“What’s the matter with him?” his friend utters, aghast. “Man, he’s a healthy dude.”
One of the nurses pushes him toward the door.“You’ll have to wait outside. We’ll let you know how he’s doing.”
The friend loiters around the exam room, peering in occasionally, asking incessantly about his companion. “Please go to the waiting room,” the nurses say, “we’ll let you know.”
The friend puts on his dark glasses and slouches out. “Man, talking to these nurses is like talking to a brick wall.”
University Hospital is the closest thing San Diego has to a county facility. Police cases — fights, auto accidents, city ambulances — uniformly come here for emergency treatment, as do drug overdoses, the indigent, MediCal patients, and any other rejects from private emergency facilities. According to one licensed vocational nurse, who got his training in Vietnam and has worked at several local hospitals, the University Hospital Emergency Room will “treat anyone,” while some hospitals “just want to know who has your insurance.” As a result of this policy, he says, the UC hospital is in trouble because it can’t collect its bills. But what counts is that it’s got “the best staff around.”
The intern calls down the hall to the psychiatrist. “Doctor. Richard’s back.”
“Tell him I’m sorry, but I can’t see him.”
Richard’s eyes protrude nervously. He stands by the door, his neck craning forward, a green T-shirt showing beneath his open jacket. He responds to the news in a staccato hiss, “You just don’t care. I need help. I’m not kidding, if something doesn’t change, I’m going to kill myself. You people are supposed to be here to help. You won’t do anything, you just don’t care.” His eyes peer dryly down the hall at the intern.
The intern begins to interrupt, fitting his statements into chinks in Richard’s bug-eyed rant.
“Richard, we can’t help you. You’ve got to help yourself. You’re not psychotic. You think you’re going to spite me by doing yourself in. If you want to do it, you won’t tell me, you’ll do it.”
Richard, tired of hearing this sort of thing, turns away and drags his tired eyes out the door. Maybe he would, maybe he wouldn’t. The intern, shaking his head, stops at a counter where a few people have gathered, watching. “What do you do for that?”someone remarks. “He wants you to do psychiatric surgery?”
“I wonder if he’ll do it,” someone else says.
The intern shrugs. One doctor lowers his magazine.“If he does, I hope he leaves the hospital first.”
The pediatrics examination room is done up in bright colors, with mobiles in the corners and a Mickey Mouse clock and Bozo the Clown grinning down from the wall in paternal reassurance. Everybody’s voices are pitched up to kiddie banter. In addition to specific treatment, the pediatricians have to be able to sway their small patients toward adult behavior, into accepting a pattern of breakdown, recovery, and lollipop reward. Mothers say, leaving,“ There now, that wasn’t so bad, was it?”
The pediatricians say their business comes in rushes. One at sunset, when the kids come home with the badges of their adventures to be discovered by mom who’d hoped they were done for the day; the second at midnight, when colds, flu, and congestion still have everybody in the house awake.“I prescribe dematol by the gallon,” a pediatrician says. “That’s the chemical name, so it’s cheaper that way. One decongestant is as good as another.”
He steps outside to join a conversation in the hall.
“I wouldn’t mind working out at the zoo. I heard about an operation they gave an orangutan there, they used the same instruments we use.”
“Well, animals get sick the same as kids.”
“Yeah, those vets have a good job, they get to work outdoors, don’t develop these flabby doctor bodies.”
“I’d like to work out at SeaWorld. I went there to apply. You’d think I could get a job with this kind of experience…No way! So many people want to work with animals.”
“Well, some of the methods might be the same, but it doesn’t just go straight across. How’d you like to treat a giraffe with the croup?”
The massive, lumpy woman wheels herself along beside the counters and desks, belittling anyone who will listen.
“You really needed that room. Oh, yeah, you really needed that room. You made me get out because you say you needed it for emergencies, and now it’s empty. You really needed that room.”
The doctors at their desks, studying the staff behind the counter,all ignore her.She persists,more volubly.
“You really needed that room.”
Finally one of the doctors breaks down.“Mrs. Grier, would you wait out front please.”
“No, I won’t wait out front. If I were a doctor and you were sick, I wouldn’t crucify you.You’re cruel.”
The doctor goes around behind her chair and tries to wheel Mrs. Grier away. She locks the brakes.
“Now come on, Mrs. Grier, let’s not be childish.”
“Let’s not anyone be childish,” she says.“I have a right to be treated like anyone else. I want to see the psychiatrist.”
“The psychiatrist doesn’t want to see you.He’s with another patient.What he’s doing is important to them, too. He can’t see you now.”
“Then you can call the police. I’m not leaving.”
A few minutes later, one of the hospital security guards rolls Mrs.Grier to a nearby phone, where she’s been promised a chance to talk to an administrative head.
“Call the police,” she cries into the phone. “I don’t care. I can’t stand the pain. It hurts. In my head, in my lungs, in my back, in my legs. I just want to be admitted.”
The crowd around the desks half-listens to the familiar scene. “I don’t believe how much time she spends around here,” one doctor says. “She’s not very well-adjusted to her disease.”
Finally, somebody upstairs agrees to admit her, and two doctors laboriously help her into a bed; service, according to their colleagues, above and beyond the call of duty. Within half an hour, she’s been released.
As she wheels herself out of the Emergency Room, she stops a few feet from the drinking fountain and, petulantly, asks the nurse to get her some water.
The nurse fills a paper cup and gives it to her. “It’s okay,” she says. “She just needs a lot of attention.”
Conversation in the ER is like anywhere else highly trained people are gathered, pressing their verbal capacities against the limits of their work, waiting to see what gets through, what comes back. For patients, it’s a matter of answering a few questions, and otherwise expressing whatever comes to mind:
“Hey, knock off the noise.”
“I want to go home.”
“Let’s move.”
“She got any clothes on?”
The conversation is detached, matter-of-fact. Without any context, caught phrases feel like bits of cold tape spliced from the cutting-room floor.
“Does anyone want to talk to Border Patrol?”
“That place full of jive women. But they got a good band.”
“Don’t go in there, ma’am, that’s not his room.”
A drunk, bitten by a cat, sits hiccupping in the corner. “This hospital takes good care of its people,” he states, and he apparently knows. Overwhelmed by gratitude, or self-pity, or just because he wants to,the drunk begins to cry. His doctor tells him, “You don’t need to come back unless this flares up. Okay? Okay?”
“Uh, okay,” the drunk sniffles.
Moments stretch into lulls, the noises pale,and talk turns to just about anything. A comic yelp comes from one of the exam rooms. “What’s the matter?” a nurse answers. “I’m having trouble taking down somebody’s pants,” the doctor calls. She ambles off. “Oh, I’m good at that.”
The man has been in a fight. He has a three-day beard, a rude purple eye, and a broken hand, which the doctor finishes wrapping. “I really think we ought to check this out further, maybe admit you,” the doctor says. The man grunts his complaint.
The doctor leaves and goes to his desk, where he consults one of his books. “It’s an odd break,” he tells one of his colleagues.
“What’s the usual mechanism of injury?”
“Direct blow to the thumb.”
After thinking it over, the doctor says, “Well, let him get dressed for now, but don’t let him leave. Orthopedics might want to take a look at him tonight — if they can do it,we’ll put him in.”
The man gets dressed, slipping an ornate black patch over his offensive eye, and wanders around the ER, waiting.
“I wonder where he got that patch,” the doctor says.
“He says he’s been injured there before,”a nurse replies. “I don’t know where you’d get a patch like that.”
Walking off, the doctor says, “He probably knows the guy who makes Hathaway shirts.”
The nurse nods her head as she finishes writing in the man’s red chart folder, then picks up another red folder and glances over at the Mexican patient it signifies. Thick bandages cover a nasty dog bite and fresh stitches. He stands with a border patrolman.
The patrolman shakes his head. “This fellow has no money or people, either in San Diego or Tijuana. He’s from Oaxaca, walked across the border. CHP saw him walking down the street, his hand dripping blood. Good thing he got across the border, because he’d be out of luck for treatment in Mexico. He’s got to come back here for treatment in a few days. They want me to keep him, but shoot, if I do, I have to charge him with something. We’ll probably give him a reentry visa and send him down to Tijuana meanwhile.”
The man stands beside the patrolman, silent, uninvolved, apparently feeling no pain. “He’d have probably ended up in LA, flopping with sixteen other guys in a two-room apartment. Not too healthy. LA spent $8 million on aliens’ hospital bills last year. They’ll never see that money.”
“Four or five hundred fellows like him get over every night. They’ll take any job they can get, any money.” He asks the man how many years of schooling he’s had. “Cuatro.” “Four,” the patrolman repeats.
On a slow night, it’s not so hard to grab a breather. There’s time for a smoke in the custodial room, standing next to somebody’s tray of half-eaten and no-longer steaming dinner. There, on the desk, a paper-bound novel lies open, broken from the many interruptions pressed into its back — Venus on the Half-Shell, it’s called.
Paradoxically, some complain that “business” is slow.“You ought to see this place under a full moon,” a receptionist tells me. “It really does make a difference.”
Another woman sits on her bed at the open door to her exam room,waiting.“It’s just this persistent cough,”she says. “They started to send me upstairs. If they’d done that, I’d be home now.”
“This way you’re ringside for the action,”the nurse tells her.
The woman gazes into the still corridor, across the idle counters. On one of them sits a copy of Physician magazine.Its cover shows a frontal view of a boy baby’s tummy and genitals, pink, robust. “Great,”the woman says, “that’s just what I need.”
On the far side of the corridor,one doctor holds an X-ray up to the light and calls to another. “Say, Gary, take a look at this — it’s really very interesting.”
It usually doesn’t take long for something to happen.
The Mexican cook sits on the examination table,soaking his hand in a bowl of sudsy water. He rolls his eyes at the ceiling and shakes his head, talking to himself in Calo, barrio slang, “Ah, I’m a dumb tortilla.”
“Let me see that finger,” the nurse asks. He takes his hand from the bowl and holds up the finger, shiny red where a sliver is missing off the end. “Sixteen years I’ve worked in kitchens, and never an accident,” he laughs. “They didn’t find this missing piece. Some customer back at the restaurant is probably eating part of my finger right now.”
Waiting.
One intern says, “This is easy work.You have a day on, and a day off.” Interns, during the year before they become a resident, do block study, a month or two at a time, in the various hospital departments, such as orthopedics or urology. The ER is one of those blocks. “There’s a lot of work when it’s there. Still, this is the easiest month.” Perhaps it’s because there’s no chance to follow every patient through a complete recovery. And the ER only functions when the doors are banging open. A lot of the time, “there’s just not that much to do.”
Four doctors are playing Hearts at one of the desks, exercising small strategies, working the odds. One has his feet propped up on the desk, showing his white socks; another taps his own knee with a reflex hammer. A few bystanders watch disaffectedly as the dealer shuffles, fanning the cards across his palm. He snaps them back into a block and flips them around the desk.
In a back room, a drunk, strapped to his bed, begins singing. Then laughing,then cursing. “He’s in here all the time,” a nurse says. “We get a lot of repeaters.”
Is she bored? “Naw. There’s a siren coming now. We can tell how bad the victim is by how soon they turn off the siren. They’re not supposed to use it within two blocks. If they use it up to the door…”
The police radio sputters and calls. “PD Ambulance to University ER. We have a bad G-I bleeder,pulse bounding, breathing labored. ETA in two.”The duty nurse acknowledges the message. “Auto-admit,” she mentions, to no one in particular.
Without instructions, the ER personnel begin to move about, preparing a room, checking instruments, phoning for special equipment. They glance at the door as they finish their cigarettes and phone calls. The receptionists lean across their counter, curious, while visitors, waiting, look around expectantly.Everyone hears the siren now, pouring through the dark residential streets around the hospital.
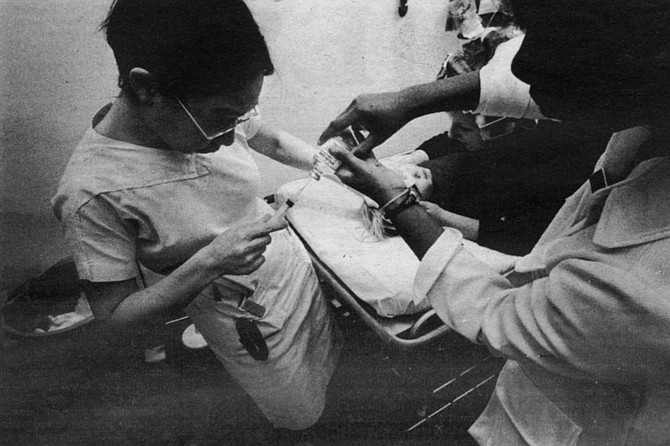
And then the gurney is rolling through the open glass doors, pushed by a police attendant, carrying a man who is bleeding freely from his gastrointestinal tract. Blood smears his cheeks and chin, and oozes through the sheets around his hips. By the time the gurney passes the receiving counter, it has picked up a nurse, then a doctor, and by the time it has crossed the corridor to Emergency Medicine, it has a small crowd around it, the man’s pulse has been taken and a portable EKG machine sent for.
Within a few minutes of entering the exam room, nearly every orifice in the man’s body has a tube in it, collecting the effluent of his ulcerating G-I tract, and everyone has been informed of the man’s medical history. He’s been hard-drinking for 25 years, his liver is shot, and his foul blood is now erupting through the soft tissue of his esophagus. He’s been bleeding for a week and hasn’t done anything about it; he’s wanted to be on his own. Now he has to be fed intravenously, the yellow fluid dripping sluggishly through the needle into his arm, and since the pain isn’t great enough to make him unconscious, has to answer questions and face the suppressed irritation of doctors who could have done something a week ago;now,maybe not.
The lines on the man’s EKG readout look like torn cardboard. “We’ve got to have blood,”one doctor states, and someone goes to call the blood bank. “Fix a spot,and let’s get him over to Emergency Surgery.”
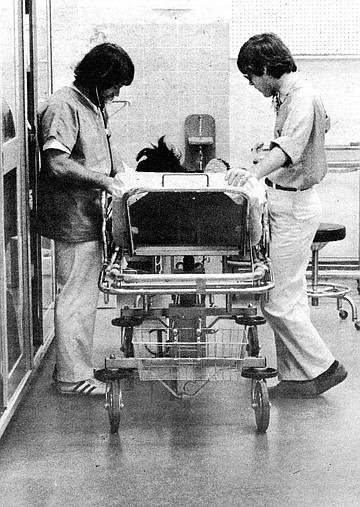
Within moments the man and his tubes have been wheeled across the hall to surgery, leaving tracks on the shiny linoleum. The nurses begin their pre-op protocol, preparing instruments and injections, checking vital functions, fluid levels, everything. They hurry back and forth between the patient and supply counter, where their conversations cross.
“This patient’s not doing too well for some reason,” one says.
“You drink that way for twenty-five years…”
“…some of the parties at nursing school.We’d be drinking grain…”
“Don’t tell tales.”
“Well, I have to make it exciting, don’t I?”
The man on his back coughs, bringing up fresh volumes of dark, sticky blood, which a nurse at his head sucks out of his mouth with a vacuum hose.
“We’re going to have to scope him,” a doctor says, and preparation began to run a scope down the man’s esophagus in order to see, with the aid of a small light, the location of the varices, the bleeding ulcers, caused by the backup of blood from his rotten liver. First, the doctors open the man’s arm and run an IV line through a main vein into his chest to monitor his heartbeat.
The man, still conscious, begins to cough.
“That’s okay, sir, you just bring it up, I’ll get it out,” the nurse at his head tells him. Then, uncontrollably, he vomits blood onto the bed, followed by gut-racking coughs of blood across the floor and onto the linen cup- board five feet away.
The surgeons have to stop working while the body shakes; the nurse calmly begins to suck up the mess with her hose.
“I’m sorry,” the man wheezes. One nurse notices the linen. “God, the cupboard door was open,” she whispers. Her stockings are splattered with red. She doesn’t stop to clean them.
“Can somebody talk to the blood bank?” a volunteer calls into the room.
“About what?” one of the doctors answers.
“About the blood.”
“Jesus.”
As the nurses and doctors work around the man, somehow not getting in each other’s way, another gurney rolls through the ER doors, across the corridor and into a room painted working white.
Nurses and a doctor drift away from the G-I bleeder to attend to the new patient, washing their hands on the way.
Their rubber-soled shoes make brisk, efficient squeaks on the shiny linoleum floor, disturbing the drunk in room six, who bangs on his bed rail and yells, “Drop dead, you prick.”
All the personnel not doing something else seem to be gathered around this one patient’s bed. Some are working, some advising, some are curious. The patient’s temperature, blood pressure, pulse, and blood sugar have been taken, and his specific difficulties are being attended to. His bed is a gymnasium of medical apparatus — tubes, wires, electrodes, bags, and bottles. His vital functions display themselves in a readout from a machine whose innards resemble the electronic workings of a satellite.
One of the interns working around the bed approaches a nurse leaning against the doorway, then turns back to the activity in the room with enthusiasm.
“Is there anything else we have to do?” he asks. She shakes her head slowly.“We don’t have to do anything.”
Here's something you might be interested in.
University Hospital's ER takes 'em all
Life, death, and in between
University Hospital's ER takes 'em all
Life, death, and in between
The police officer pushes his prisoner, locked in a wheelchair, through the Emergency Room doors. The man, a well-dressed scuffler, sits with his head on his chest and says nothing as the officer checks in at the front desk. The
officer then wheels the chair through Emergency Surgery and into an examination room in Emergency Medicine, where he locks the man to his bed.
“We caught him inside a department store where we’ve had around $125,000 in burglaries lately,” the officer says. “His modus operandi fits the pattern. The burglar hides in the store just before closing, under a bed or something, then when everybody’s gone, he’ll get up, get the stuff he wants, no more than he can run with, throw a chair through a window, and break out. It takes us a few minutes to get there, wherever we are, so he might get away. But this guy set off a silent alarm in the fur locker.”
The prisoner’s chains rattle and the officer ducks into the room.“I want to take off my coat,” the man says.
The officer unlocks the cuffs and, stiff-armed, helps the prisoner with his coat, keeping one hand at his gun-side. When the coat is off, he locks the man to his bed again.
“What did you bring him to the ER for?” the nurse asks.
“Says he’s sick. Says he passed out and just woke up. He called our dispatcher about the same time we were pulling into the parking lot and said he was locked in the store. I don’t know if he’s the one we’ve been looking for. But the fur locker’s one floor down and the other side of the building from where he says he passed out. He’s got a record, too. How does he look to you?” he asked the nurse.
She shrugs.“Most of the ones you bring in are frauds. ‘Chest pains’ and ‘fainting.’ I know you’re obligated by law to bring the guy here if he says he’s sick. Oh, well, it buys him some time, and he gets a free checkup. Besides,” she adds, “we might find something.”
The Emergency Room at University Hospital greets its patients with the neutrality of a business office. They walk or roll or are carried through its pneumatic glass doors into the familiar atmosphere of nothing special: forms to sign and phones and IBM cash registers going tacka-tack. The doctors are rarely dressed in surgical white; they wear, instead, striped shirts, bow ties, Wallabees. The centrifuge in the back room, with its little vials of blood spinning out and around, whirs constantly, but it could as easily be the sound of a vacuum cleaner or Star Trek on a faraway television, and the sound blends easily with the hum of small talk.
The walls are white. Not a clinical white, but working white, trimmed with hard, bright red, violet, and orange at the doors and counters.
If you were to wake up here, staring at the tiny holes in the ceiling tile and wondering where you were, you might simply think you were in a freshly painted room. You’d probably never guess that the only hint of a smell was wet cast plaster.
You might think you hadn’t been noticed. But someone sees you from the corner of their eye and asks if there’s anything they can do.
The ambulance radio announces a fight victim coming in. Two minutes later the victim rolls through the door, his jean jacket and clothing stuffed on the rack below the gurney. Except for his eyes, which he opens and closes slowly, halfway, he doesn’t move. His friend, in jeans and jacket, with a wine bota slung over his shoulder, walks alongside.“You’re going to be okay, man. You just take it easy, okay?” The man on the gurney, already being wheeled into the emergency surgery exam room, doesn’t answer.
Nurses help the man onto an examination table. A pulpy blue wound covers his forehead and he moves his body sluggishly. While they inventory his personal belongings, nurses and staff try to coax his name, his cooperation, any response from him. He doesn’t talk, only opens and closes his eyes.
When the doctor comes, he asks the man what has happened. The man moves his lips, but no sound comes out. “Have you been taking any drugs?” the doctor asks, then turns to the man’s friend, watching from the doorway. “Has he done any drugs tonight?”
“Just a couple of brews. Maybe a quart...”
The doctor turns back to the table.“Put your tongue out. Okay, now show me all your teeth.”
The friend walks around to the head of the exam table. “Say something, man.” No answer. “Hey, is he going to be all right?”
“What happened to him?” the doctor asks.
“These guys jumped him in Horton Plaza. Two big guys, man, for no reason. I can’t believe this — he’s a healthy dude.”
The doctor returns to his patient.“Can you lift your feet? Good. It’s important that you answer the questions, all right?” The doctor presses his fingers around the forehead wound. “This hurt? This?” Suddenly the man lurches upright, shouting, “Hey, man, hey, man,” groping in the air.
“What’s the matter with him?” his friend utters, aghast. “Man, he’s a healthy dude.”
One of the nurses pushes him toward the door.“You’ll have to wait outside. We’ll let you know how he’s doing.”
The friend loiters around the exam room, peering in occasionally, asking incessantly about his companion. “Please go to the waiting room,” the nurses say, “we’ll let you know.”
The friend puts on his dark glasses and slouches out. “Man, talking to these nurses is like talking to a brick wall.”
University Hospital is the closest thing San Diego has to a county facility. Police cases — fights, auto accidents, city ambulances — uniformly come here for emergency treatment, as do drug overdoses, the indigent, MediCal patients, and any other rejects from private emergency facilities. According to one licensed vocational nurse, who got his training in Vietnam and has worked at several local hospitals, the University Hospital Emergency Room will “treat anyone,” while some hospitals “just want to know who has your insurance.” As a result of this policy, he says, the UC hospital is in trouble because it can’t collect its bills. But what counts is that it’s got “the best staff around.”
The intern calls down the hall to the psychiatrist. “Doctor. Richard’s back.”
“Tell him I’m sorry, but I can’t see him.”
Richard’s eyes protrude nervously. He stands by the door, his neck craning forward, a green T-shirt showing beneath his open jacket. He responds to the news in a staccato hiss, “You just don’t care. I need help. I’m not kidding, if something doesn’t change, I’m going to kill myself. You people are supposed to be here to help. You won’t do anything, you just don’t care.” His eyes peer dryly down the hall at the intern.
The intern begins to interrupt, fitting his statements into chinks in Richard’s bug-eyed rant.
“Richard, we can’t help you. You’ve got to help yourself. You’re not psychotic. You think you’re going to spite me by doing yourself in. If you want to do it, you won’t tell me, you’ll do it.”
Richard, tired of hearing this sort of thing, turns away and drags his tired eyes out the door. Maybe he would, maybe he wouldn’t. The intern, shaking his head, stops at a counter where a few people have gathered, watching. “What do you do for that?”someone remarks. “He wants you to do psychiatric surgery?”
“I wonder if he’ll do it,” someone else says.
The intern shrugs. One doctor lowers his magazine.“If he does, I hope he leaves the hospital first.”
The pediatrics examination room is done up in bright colors, with mobiles in the corners and a Mickey Mouse clock and Bozo the Clown grinning down from the wall in paternal reassurance. Everybody’s voices are pitched up to kiddie banter. In addition to specific treatment, the pediatricians have to be able to sway their small patients toward adult behavior, into accepting a pattern of breakdown, recovery, and lollipop reward. Mothers say, leaving,“ There now, that wasn’t so bad, was it?”
The pediatricians say their business comes in rushes. One at sunset, when the kids come home with the badges of their adventures to be discovered by mom who’d hoped they were done for the day; the second at midnight, when colds, flu, and congestion still have everybody in the house awake.“I prescribe dematol by the gallon,” a pediatrician says. “That’s the chemical name, so it’s cheaper that way. One decongestant is as good as another.”
He steps outside to join a conversation in the hall.
“I wouldn’t mind working out at the zoo. I heard about an operation they gave an orangutan there, they used the same instruments we use.”
“Well, animals get sick the same as kids.”
“Yeah, those vets have a good job, they get to work outdoors, don’t develop these flabby doctor bodies.”
“I’d like to work out at SeaWorld. I went there to apply. You’d think I could get a job with this kind of experience…No way! So many people want to work with animals.”
“Well, some of the methods might be the same, but it doesn’t just go straight across. How’d you like to treat a giraffe with the croup?”
The massive, lumpy woman wheels herself along beside the counters and desks, belittling anyone who will listen.
“You really needed that room. Oh, yeah, you really needed that room. You made me get out because you say you needed it for emergencies, and now it’s empty. You really needed that room.”
The doctors at their desks, studying the staff behind the counter,all ignore her.She persists,more volubly.
“You really needed that room.”
Finally one of the doctors breaks down.“Mrs. Grier, would you wait out front please.”
“No, I won’t wait out front. If I were a doctor and you were sick, I wouldn’t crucify you.You’re cruel.”
The doctor goes around behind her chair and tries to wheel Mrs. Grier away. She locks the brakes.
“Now come on, Mrs. Grier, let’s not be childish.”
“Let’s not anyone be childish,” she says.“I have a right to be treated like anyone else. I want to see the psychiatrist.”
“The psychiatrist doesn’t want to see you.He’s with another patient.What he’s doing is important to them, too. He can’t see you now.”
“Then you can call the police. I’m not leaving.”
A few minutes later, one of the hospital security guards rolls Mrs.Grier to a nearby phone, where she’s been promised a chance to talk to an administrative head.
“Call the police,” she cries into the phone. “I don’t care. I can’t stand the pain. It hurts. In my head, in my lungs, in my back, in my legs. I just want to be admitted.”
The crowd around the desks half-listens to the familiar scene. “I don’t believe how much time she spends around here,” one doctor says. “She’s not very well-adjusted to her disease.”
Finally, somebody upstairs agrees to admit her, and two doctors laboriously help her into a bed; service, according to their colleagues, above and beyond the call of duty. Within half an hour, she’s been released.
As she wheels herself out of the Emergency Room, she stops a few feet from the drinking fountain and, petulantly, asks the nurse to get her some water.
The nurse fills a paper cup and gives it to her. “It’s okay,” she says. “She just needs a lot of attention.”
Conversation in the ER is like anywhere else highly trained people are gathered, pressing their verbal capacities against the limits of their work, waiting to see what gets through, what comes back. For patients, it’s a matter of answering a few questions, and otherwise expressing whatever comes to mind:
“Hey, knock off the noise.”
“I want to go home.”
“Let’s move.”
“She got any clothes on?”
The conversation is detached, matter-of-fact. Without any context, caught phrases feel like bits of cold tape spliced from the cutting-room floor.
“Does anyone want to talk to Border Patrol?”
“That place full of jive women. But they got a good band.”
“Don’t go in there, ma’am, that’s not his room.”
A drunk, bitten by a cat, sits hiccupping in the corner. “This hospital takes good care of its people,” he states, and he apparently knows. Overwhelmed by gratitude, or self-pity, or just because he wants to,the drunk begins to cry. His doctor tells him, “You don’t need to come back unless this flares up. Okay? Okay?”
“Uh, okay,” the drunk sniffles.
Moments stretch into lulls, the noises pale,and talk turns to just about anything. A comic yelp comes from one of the exam rooms. “What’s the matter?” a nurse answers. “I’m having trouble taking down somebody’s pants,” the doctor calls. She ambles off. “Oh, I’m good at that.”
The man has been in a fight. He has a three-day beard, a rude purple eye, and a broken hand, which the doctor finishes wrapping. “I really think we ought to check this out further, maybe admit you,” the doctor says. The man grunts his complaint.
The doctor leaves and goes to his desk, where he consults one of his books. “It’s an odd break,” he tells one of his colleagues.
“What’s the usual mechanism of injury?”
“Direct blow to the thumb.”
After thinking it over, the doctor says, “Well, let him get dressed for now, but don’t let him leave. Orthopedics might want to take a look at him tonight — if they can do it,we’ll put him in.”
The man gets dressed, slipping an ornate black patch over his offensive eye, and wanders around the ER, waiting.
“I wonder where he got that patch,” the doctor says.
“He says he’s been injured there before,”a nurse replies. “I don’t know where you’d get a patch like that.”
Walking off, the doctor says, “He probably knows the guy who makes Hathaway shirts.”
The nurse nods her head as she finishes writing in the man’s red chart folder, then picks up another red folder and glances over at the Mexican patient it signifies. Thick bandages cover a nasty dog bite and fresh stitches. He stands with a border patrolman.
The patrolman shakes his head. “This fellow has no money or people, either in San Diego or Tijuana. He’s from Oaxaca, walked across the border. CHP saw him walking down the street, his hand dripping blood. Good thing he got across the border, because he’d be out of luck for treatment in Mexico. He’s got to come back here for treatment in a few days. They want me to keep him, but shoot, if I do, I have to charge him with something. We’ll probably give him a reentry visa and send him down to Tijuana meanwhile.”
The man stands beside the patrolman, silent, uninvolved, apparently feeling no pain. “He’d have probably ended up in LA, flopping with sixteen other guys in a two-room apartment. Not too healthy. LA spent $8 million on aliens’ hospital bills last year. They’ll never see that money.”
“Four or five hundred fellows like him get over every night. They’ll take any job they can get, any money.” He asks the man how many years of schooling he’s had. “Cuatro.” “Four,” the patrolman repeats.
On a slow night, it’s not so hard to grab a breather. There’s time for a smoke in the custodial room, standing next to somebody’s tray of half-eaten and no-longer steaming dinner. There, on the desk, a paper-bound novel lies open, broken from the many interruptions pressed into its back — Venus on the Half-Shell, it’s called.
Paradoxically, some complain that “business” is slow.“You ought to see this place under a full moon,” a receptionist tells me. “It really does make a difference.”
Another woman sits on her bed at the open door to her exam room,waiting.“It’s just this persistent cough,”she says. “They started to send me upstairs. If they’d done that, I’d be home now.”
“This way you’re ringside for the action,”the nurse tells her.
The woman gazes into the still corridor, across the idle counters. On one of them sits a copy of Physician magazine.Its cover shows a frontal view of a boy baby’s tummy and genitals, pink, robust. “Great,”the woman says, “that’s just what I need.”
On the far side of the corridor,one doctor holds an X-ray up to the light and calls to another. “Say, Gary, take a look at this — it’s really very interesting.”
It usually doesn’t take long for something to happen.
The Mexican cook sits on the examination table,soaking his hand in a bowl of sudsy water. He rolls his eyes at the ceiling and shakes his head, talking to himself in Calo, barrio slang, “Ah, I’m a dumb tortilla.”
“Let me see that finger,” the nurse asks. He takes his hand from the bowl and holds up the finger, shiny red where a sliver is missing off the end. “Sixteen years I’ve worked in kitchens, and never an accident,” he laughs. “They didn’t find this missing piece. Some customer back at the restaurant is probably eating part of my finger right now.”
Waiting.
One intern says, “This is easy work.You have a day on, and a day off.” Interns, during the year before they become a resident, do block study, a month or two at a time, in the various hospital departments, such as orthopedics or urology. The ER is one of those blocks. “There’s a lot of work when it’s there. Still, this is the easiest month.” Perhaps it’s because there’s no chance to follow every patient through a complete recovery. And the ER only functions when the doors are banging open. A lot of the time, “there’s just not that much to do.”
Four doctors are playing Hearts at one of the desks, exercising small strategies, working the odds. One has his feet propped up on the desk, showing his white socks; another taps his own knee with a reflex hammer. A few bystanders watch disaffectedly as the dealer shuffles, fanning the cards across his palm. He snaps them back into a block and flips them around the desk.
In a back room, a drunk, strapped to his bed, begins singing. Then laughing,then cursing. “He’s in here all the time,” a nurse says. “We get a lot of repeaters.”
Is she bored? “Naw. There’s a siren coming now. We can tell how bad the victim is by how soon they turn off the siren. They’re not supposed to use it within two blocks. If they use it up to the door…”
The police radio sputters and calls. “PD Ambulance to University ER. We have a bad G-I bleeder,pulse bounding, breathing labored. ETA in two.”The duty nurse acknowledges the message. “Auto-admit,” she mentions, to no one in particular.
Without instructions, the ER personnel begin to move about, preparing a room, checking instruments, phoning for special equipment. They glance at the door as they finish their cigarettes and phone calls. The receptionists lean across their counter, curious, while visitors, waiting, look around expectantly.Everyone hears the siren now, pouring through the dark residential streets around the hospital.
And then the gurney is rolling through the open glass doors, pushed by a police attendant, carrying a man who is bleeding freely from his gastrointestinal tract. Blood smears his cheeks and chin, and oozes through the sheets around his hips. By the time the gurney passes the receiving counter, it has picked up a nurse, then a doctor, and by the time it has crossed the corridor to Emergency Medicine, it has a small crowd around it, the man’s pulse has been taken and a portable EKG machine sent for.
Within a few minutes of entering the exam room, nearly every orifice in the man’s body has a tube in it, collecting the effluent of his ulcerating G-I tract, and everyone has been informed of the man’s medical history. He’s been hard-drinking for 25 years, his liver is shot, and his foul blood is now erupting through the soft tissue of his esophagus. He’s been bleeding for a week and hasn’t done anything about it; he’s wanted to be on his own. Now he has to be fed intravenously, the yellow fluid dripping sluggishly through the needle into his arm, and since the pain isn’t great enough to make him unconscious, has to answer questions and face the suppressed irritation of doctors who could have done something a week ago;now,maybe not.
The lines on the man’s EKG readout look like torn cardboard. “We’ve got to have blood,”one doctor states, and someone goes to call the blood bank. “Fix a spot,and let’s get him over to Emergency Surgery.”
Within moments the man and his tubes have been wheeled across the hall to surgery, leaving tracks on the shiny linoleum. The nurses begin their pre-op protocol, preparing instruments and injections, checking vital functions, fluid levels, everything. They hurry back and forth between the patient and supply counter, where their conversations cross.
“This patient’s not doing too well for some reason,” one says.
“You drink that way for twenty-five years…”
“…some of the parties at nursing school.We’d be drinking grain…”
“Don’t tell tales.”
“Well, I have to make it exciting, don’t I?”
The man on his back coughs, bringing up fresh volumes of dark, sticky blood, which a nurse at his head sucks out of his mouth with a vacuum hose.
“We’re going to have to scope him,” a doctor says, and preparation began to run a scope down the man’s esophagus in order to see, with the aid of a small light, the location of the varices, the bleeding ulcers, caused by the backup of blood from his rotten liver. First, the doctors open the man’s arm and run an IV line through a main vein into his chest to monitor his heartbeat.
The man, still conscious, begins to cough.
“That’s okay, sir, you just bring it up, I’ll get it out,” the nurse at his head tells him. Then, uncontrollably, he vomits blood onto the bed, followed by gut-racking coughs of blood across the floor and onto the linen cup- board five feet away.
The surgeons have to stop working while the body shakes; the nurse calmly begins to suck up the mess with her hose.
“I’m sorry,” the man wheezes. One nurse notices the linen. “God, the cupboard door was open,” she whispers. Her stockings are splattered with red. She doesn’t stop to clean them.
“Can somebody talk to the blood bank?” a volunteer calls into the room.
“About what?” one of the doctors answers.
“About the blood.”
“Jesus.”
As the nurses and doctors work around the man, somehow not getting in each other’s way, another gurney rolls through the ER doors, across the corridor and into a room painted working white.
Nurses and a doctor drift away from the G-I bleeder to attend to the new patient, washing their hands on the way.
Their rubber-soled shoes make brisk, efficient squeaks on the shiny linoleum floor, disturbing the drunk in room six, who bangs on his bed rail and yells, “Drop dead, you prick.”
All the personnel not doing something else seem to be gathered around this one patient’s bed. Some are working, some advising, some are curious. The patient’s temperature, blood pressure, pulse, and blood sugar have been taken, and his specific difficulties are being attended to. His bed is a gymnasium of medical apparatus — tubes, wires, electrodes, bags, and bottles. His vital functions display themselves in a readout from a machine whose innards resemble the electronic workings of a satellite.
One of the interns working around the bed approaches a nurse leaning against the doorway, then turns back to the activity in the room with enthusiasm.
“Is there anything else we have to do?” he asks. She shakes her head slowly.“We don’t have to do anything.”
Comments