{kind=link}
Here's something you might be interested in.
Ask a Hipster — Advice you didn't know you needed
Big Screen — Movie commentary
Blurt — Music's inside track
Booze News — San Diego spirits
Classical Music — Immortal beauty
Classifieds — Free and easy
Close to Home — What it’s like on the street where you live
Cover Stories — Front-page features
Drinks All Around — Bartenders' drink recipes
Excerpts — Literary and spiritual excerpts
Feast! — Food & drink reviews
Feature Stories — Local news & stories
Fishing Report — What’s getting hooked from ship and shore
From the Archives — Spotlight on the past
Golden Dreams — Talk of the town
The Gonzo Report — Making the musical scene, or at least reporting from it
Letters — Our inbox
Movies@Home — Local movie buffs share favorites
Movie Reviews — Our critics' picks and pans
Musician Interviews — Up close with local artists
Neighborhood News from Stringers — Hyperlocal news
News Ticker — News & politics
Obermeyer — San Diego politics illustrated
Outdoors — Weekly changes in flora and fauna
Overheard in San Diego — Eavesdropping illustrated
Poetry — The old and the new
Reader Travel — Travel section built by travelers
Reading — The hunt for intellectuals
Roam-O-Rama — SoCal's best hiking/biking trails
San Diego Beer — Inside San Diego suds
SD on the QT — Almost factual news
Sheep and Goats — Places of worship
Special Issues — The best of
Street Style — San Diego streets have style
Surf Diego — Real stories from those braving the waves
Theater — On stage in San Diego this week
Tin Fork — Silver spoon alternative
Under the Radar — Matt Potter's undercover work
Unforgettable — Long-ago San Diego
Unreal Estate — San Diego's priciest pads
Your Week — Daily event picks
UCSD shows exactly what gall bladder surgery is like
Under the knife
More than 20 million people in the US have gallstones in their gallbladders.
Two rubber-veiled hands press cloths down; the pumpkin square of abdomen shines taut. Framing the exposed area, faded aqua drapes conceal curves of body. Another sheathed hand grasps a silver blade, angles it with delicacy toward the skin. The blade is glided in deeply. There is no dramatic pause before that shock of knife in skin.

“Gallstones are the tombstones of infection,” goes one maxim.
For seven inches, the scalpel is drawn across the orange patch of flesh, right through. Concealed by the faded sheets, it is not a man who has been slit open, but a vessel temporarily commandeered by science. For the two hours this cholecystectomy will take, the body has no gestures, no language of its own.

The surgeons squinted at the bluish ghosts of organs on a viewing screen.
Historical medical literature, dating as far back as the days of the Talmud, reveals a knowledge of gallbladder disease and gallstones. As the human diet became more complex, cholecystitis and cholethiasis became more common. Richer, fattier foods and a sedentary lifestyle made the gallbladder function less efficiently and, consequently, more prone to form gallstones. Today, gallbladder disease and gallstones are common complaints.

A hand holding the forceps grasps a tip of the liver’s lower edge, lifting it gingerly, revealing the gallbladder, nestled against the liver’s back.
The man whose body lay pale and naked in UCSD Medical Center’s Operating Room 3 suffered from increasingly frequent attacks of pain, the result of gallstones. As in almost all cases of surgery for gallstones, the man’s entire gallbladder was to be removed. Cholecystectomy is considered a major operation but not a dangerous one. The mortality rate is less than one percent. Fatalities mostly occur in very complicated cases or in people who seek treatment too late.

It is 11:27, and LEDs on the ventilator show the body’s pulse is 50, blood pressure 135/81.
Half an hour before the first incision, the patient’s process of subjugation had already begun.
The surgery ward was slightly shabby, peeling blue paint on the doorjambs. Room 3 smelled of nothing — a sterile smell.
Five, six threads radiate up at each side of the seam, resembling the hoisted oars of a Viking ship.
One wall was covered with metal screens to ventilate the room with “relatively germ-free” air, said the scrub nurse. In the center of the roughly 15-foot-square room was the gurney and, motionless on it, the patient. His flesh was pasty in the cold light. Sparse dark brown hair on his groin, abdomen, and arms. At his head, the anesthesiologist -made adjustments on an array of machines: blood pressure, heart rate, blood oxygen level, breathing patterns are monitored. An EEG monitor to read his brain waves. At the body’s feet, a mobile steel basin on a pedestal contained a silver pitcher standing in several inches of saline solution. The silver pitcher held what looked like a meat baster — a bulb irrigator, also filled with saline. The aqua-suited surgical team talked easily as they made their routine preparations. In the presence of this man sleeping, penis exposed, their informality seemed almost callous.
The man’s grayish face was vised in tubes and tape. The tubes attached him to a mechanical ventilator animated by flashing LEDs and hissing sounds. A long line of esophageal stethoscope disappeared into his mouth at one end and into the anesthesiologist’s left ear at the other end. The patient’s eyes had been lubricated and sealed shut with surgical tape. He looked dead. At his temples, electrical clips on white adhesive disks, as if his head were a car battery to be charged. The anesthesiologist, standing behind the head, threaded a long curve of nasogastric tube into the nose, through which the stomach’s contents would exit. A probe was inserted into one of the patient’s fingertips, a pulse oximeter, to measure the oxygen level in his blood. His mouth was taped around a small plastic frame. Attached in the frame, a corrugated endotracheal tube from the ventilator brought his lungs a mixture of 43 percent oxygen and 55 percent nitrous oxide and isoflurane. The ventilator deflated his lungs again, measured via a capnograph the carbon dioxide leaving his lungs, breathed more oxygen and nitrous oxide and isoflurane into him. Through an IV in one arm, a mixture of sodium Pentothal and morphine entered his blood stream. The anesthesiologist injected him with vecuronium, a neuromuscular relaxant that would seduce his muscles into admitting the surgeon’s knife with little resistance.
A nurse unwrapped a plastic tube attached to a brown rubber coupling. She winced, then swiftly jammed it into the opening of the patient’s urethra. Seconds later, a small stream of golden urine slid slowly down the tube to a plastic bag lying on the floor. The nurse squatted down, nudged the bag under the edge of the gurney. A surgeon with a disposable razor shaved the coarse hair from the patient’s abdomen. Tearing off a wide swatch of adhesive from a roll, he daubed up the loose hairs from the shorn belly. A nurse drew up a sheet, worn soft, over the patient’s legs. As if in afterthought, she settled a white towel over the small, curled penis.
A large x-ray machine was wheeled in, and the room was cleared for the procedure. The team members stood in the hallway, talking shop. A nurse passing down the hall paused to chat with the scrub nurse: “You still here?” “Yeah.” “Whatcha doing?” “Gallbladder.” “Yeah?” “You on tonight?” "Yeah.”
Five minutes later, the surgeons squinted at the bluish ghosts of organs on a viewing screen. The gallbladder was a dwarf on the biliary tree, nearly obscured by the ovals of liver, pancreas, kidney, and adrenal gland.
In the center of the room, a nurse positioned a tray of Betadine solution and sponges on wooden sticks at the body’s side. She stroked the clammy stomach with frothy reddish-brown liquid, wiped it away again. Six times with soap, three times with Betadine, to make the skin as sterile as possible. The give of skin under the swab’s pressure briefly made the body seem tender and alive.
A length of plastic wrap, orange with Betadine, was rolled over the hairless, pale brown abdomen and pressed smooth. Faded aqua cloths were draped over the body, leaving the plastic-covered area exposed. The edges were taped and covered with gauzy white towels. The anesthesiologist raised a metal frame on either side of the neck and slipped an aqua curtain between the two poles. The body lay visually decapitated.
Gallbladder disease is generally caused by a bacterial infection, resulting in acute or chronic inflammation — like infections of the appendix, tonsils, or any other organ. If the gallbladder is inflamed, the blood supply to its walls may be restricted, and the gallbladder may fill with pus, even become gangrenous.
In some cases, though it is not known why, chronic inflammation causes gallstones. Disease can also result from a functional disturbance — the gallbladder failing to empty when it is called upon to secrete bile — or a chemical disturbance, causing stones to leave the bile and possibly obstruct its flow. A stone in the cystic duct, which runs between the gallbladder and the common bile duct, is most often the cause of inflammation.
High body temperature, pain and tenderness near the gallbladder, and an elevated white blood cell count all indicate acute inflammation. A gallbladder operation is then imperative. The pain of the inflammation is said to be dull and deep, shifting when you change position.
The cystic duct normally has the diameter of a pencil. When the gallbladder contracts during the digestive process, any stone (usually larger than the duct) would be forced into this tube. Eventually, the stone either drops back into the gallbladder and the attack subsides; remains stuck, producing acute infection requiring more or less immediate surgery, or passes on through the cystic duct into the common bile duct, possibly lodging at the juncture of the two. Should the latter take place, the entire flow of bile is obstructed, causing jaundice.
Before finally undergoing cholecystectomy, the afflicted person may contend with chronic indigestion, bloating, heartburn, nausea, flatulence, “excruciatingly knifelike” pain shooting from the upper abdomen straight up through the right shoulder, and jaundice. Cholecystatic diseases are also often accompanied by pruritus — itching — a source of severe discomfort in some cases. Pruritus usually appears about the same time as jaundice or a little before it. The itching is most severe on the extremities and is aggravated by warm, humid weather. Once thought to correspond to the levels of bile salts in the skin, the cause of the pruritus remains obscure.
If an operation is not performed, jaundice can persist, and the patient may eventually die from the toxic effects of the bile build-up. Unchecked inflammation can result in gangrene or a rupture of the organ. Either of these eventualities can cause fatal peritonitis unless immediate surgery is performed. Cancer of the gallbladder develops in approximately one to two percent of those patients who have chronic gallbladder inflammation with stones.
More than 20 million people in the US have gallstones in their gallbladders. It is estimated that approximately 25 percent of all women and 10 percent of all men will develop gallstones at some time or other before they reach 60 years of age. About 300,000 operations are performed annually for this disease, and at least 6000 deaths result from its complications or treatment. The possibility of gallbladder disease rises with age.
Cholesterol gallstones are found most often in American Indians. Frequency is lower in whites, and lowest in blacks. More than 75 percent of American Indian women over age 40 are affected. Before puberty, the disease is rare but equally frequent in both sexes. Between the ages of about 35 and 55, women are affected with three times the frequency of men. Hormonal changes caused by pregnancy, and the use of oral contraceptives, may be responsible for its greater frequency in women. After menopause, however, the disparity in gallstone incidence between men and women narrows.
The formation of gallstones is a mystery. The prevalent theory is that an upset in a patient’s chemistry — specifically, failure of fat and cholesterol metabolism — causes stones to crystallize and separate out from the fluid bile. Another theory is that stones are the aftermath of previous infection which may have occurred many years before. “Gallstones are the tombstones of infection,” goes one maxim.
Stones can vary in size from a millet seed to a hen’s egg. There is no correlation between the number and size of the stones and the symptoms they produce. Sometimes a single small stone can cause more trouble than a large one or many jagged ones.
The gallstones in 75 percent of patients are composed predominantly of cholesterol and are called cholesterol stones. The remaining 25 percent are pigment stones. Regardless of composition, the gallstones have similar consequences.
Cholesterol gallstones result when the liver secretes bile that is supersaturated with cholesterol. Influenced by unknown factors present in bile, the cholesterol separates from solution. It is thought that in the calm harbor of the gallbladder, small grains of pigment, called nidi, join the crystals, along with a mucoprotein paste. The newly formed crystals grow into stones of a size easily visible with the naked eye. They sometimes make their way out of the gallbladder in bile, lodging in the nearby ducts.
Pigment stones account for 25 percent of gallstones in the US and 60 percent of those in Japan. They are black, sometimes dark brown, 2 to 5 mm in diameter. Their frequency is similar in men and women, and in blacks and whites, but rare in American Indians. Cirrhosis, bile blockage due to a dilated common duct, and chronic hemolysis (the breaking apart of red blood corpuscles) are favorable conditions for pigment-stone formation. About 90 percent of pigment stones are composed of dense mixtures of bacteria with the pigment solids. It is speculated that bacteria could have a primary role in pigment gallstone formation, which would help to explain why people with pigment gallstones develop sepsis (toxicity caused by the absorption of bacteria into the blood stream) more often than do those with cholesterol gallstones.
The mere existence of stones doesn’t necessitate immediate surgery, but it is often suggested as a means to avoid future complications. It is believed there are many people living comfortably with gallbladders filled with stones who never develop symptoms.
In the US, only about 30 percent of people with cholelithiasis end up in surgery. Each year, about two percent of those with asymptomatic gallstones develop symptoms.
The tendency is to operate on younger patients and “temporize” in the elderly.
Little is audible above 11 the vacant whoosh of the ventilator. A high tone marks the rhythm of the patient's heart, adding a theatrical tension to the proceedings. There is no clinking of metal heard as a nurse fusses with a tray of tools overhanging the aqua-draped legs. Mumbles from behind six face masks direct the movements of twelve hands.
The white cotton cloths around the incision seep red as a surgeon’s hands push down. Under the pressure of the antiseptic plastic wrap stretched over the abdomen, the opened skin springs back, revealing a garish-pink layer of fat.
“Okay, we’re in.” A surgeon hands over his metal instrument, takes the yellow plastic pencil that a nurse hands him. A delicate silver point projects from the pencil’s tip. The other end is attached by a yellow plastic cord to a low-standing machine. A dial on the machine reads: scalpel, 35 watts. The surgeon braces one beige rubber wrist against the body’s right hipbone. He draws the yellow “hot knife” shallowly through the fat, tracing the incision. Wisps of smoke curl up, catching the light from the surgical lamps focused on the work. The odor of scorched skin rises. “Smells like barbecue, doesn’t it?” says a nurse.
As the beige hands draw the yellow pencil again and again, the cauterized fat parts. A gorge is formed. Periodically, the pencil is removed and wiped against an abrasive pad on the pencil’s yellow plastic holster, lying on the body’s shoulder. Tiny shreds of tissue cling to the abrasive surface. Another hand lowers a suction tube down, holds it against one suety wall. The walls of the gorge are formed of glossy curds, deep pink. The rubber hands descend into the ravine, stroking the fat apart. The valley widens as gauzy white cloths are firmed against the walls. The exertion raises bluish tendons up under the rubber gloves.
Another surgeon enters the room. A nurse draws gloves over his damp, upheld hands, pulls a knit-cuffed gown up his arms and cinches it at his back. The surgeon moves to the table, leans against the body’s hip to peer at the crevice of flesh and jelly. The surgeon with the hot knife backsteps, ceding his place to the newcomer. The movement is precise and elegant. Beneath the fat, a thin taut skin is now visible: the fascia, a layer of muscles and the tissues that connect them. The fascia is sheer and white; cords of pinkness cross the dark mass beneath. The surgical field is perhaps five inches wide and visible through the complete length of the incision. A nurse hands the surgeon a saline-filled bulb irrigator. Solution is squirted against the pale membrane, and the suction tube dives down to draw up a liquid the color of strawberry Kool-Aid. Beads of it hurry along the crystalline plastic suction tube toward a container next to the ventilator. The beads catch the surgical lamps’ glare, dazzling as rubies.
Very close to the open body, there is a vague warm scent, nearly overpowered by the Betadined stomach. It is the smell of sex, fertility — light and sweet and rich with blood. A surgeon lowers the electrocautery pencil between the three-inch pink walls, draws it down the fascia. As the thin tissue springs.apart, saline solution is quickly squirted in the rift, into which the suction tube swoops again to draw up in its beak. The yellow pencil is withdrawn. Another surgeon cups a curving silver spatula inside, against the wall of fat, coaxing it back.
The organs look like stones on a creek bottom. They lie with flat sides upward — the sherbet-orange surface of the pancreas tucks under a beige curve of a kidney. The liver, slightly to the left as one faces across the body, is deep mauve. The organs are smooth and glistening. Two pairs of hands push wedges of white cloth in to hold the fat layer at bay. A hand holding the forceps grasps a tip of the liver’s lower edge, lifting it gingerly, revealing the gallbladder, nestled against the liver’s back. Another pair of forceps in another hand takes hold of the gallbladder’s lower end, pulls it gently down into view. In size and shape, it resembles a pickled white pear, with a pink and blue lace just beneath its surface.
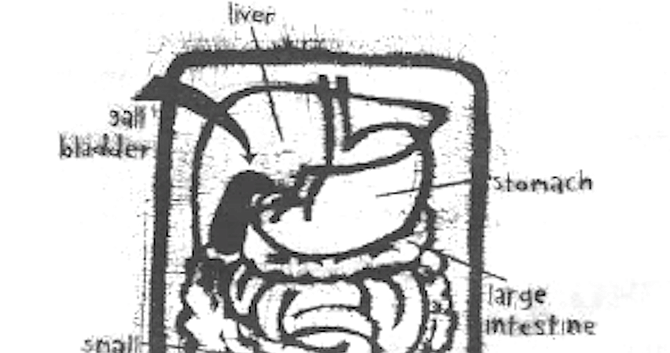
The gallbladder is a small sac, lying partially attached to the underside of the liver, in the groove between its two lobes, in the upper right portion of the abdomen. Located just beneath the arch of the ribs, it connects at its bulbous top with the liver by means of the two hepatic ducts. The sac’s narrow end connects with the top of the duodenum (the first part of small intestine) via the cystic duct, which meets the common bile duct.
This small organ’s function is to store and concentrate the bile produced and secreted by the liver. It holds about 50 ml. of bile when full. When food is eaten, particularly fatty food, the gallbladder contracts and a sphincter at the end of the common duct relaxes. During the moments when the pressure in the duct exceeds the sphincter’s resistance, bile is forced into the duodenum in squirts. The intestine will receive a supply of diluted bile directly from the liver, as well. It is essential for the digestion of fats and fatlike substances.
The gallbladder’s mucous membrane is thrown into prominent ridges when the organ is collapsed. The ridges flatten when the gallbladder is distended. Tall columns of cells form the gallbladder’s mucous membrane and are covered by hairlike microvilli on one side.
Wide channels separate the individual cells. The connecting ducts’ walls contain only small amounts of smooth muscle, except for the sphincter ringing the end of the common duct. The gallbladder musculature is made of interlocking bundles of long and spiraling fibers.
A ligament holds the internal organs in place from liver to duodenum. There is an artery to the left of the common duct and a vein, the portal vein, lying behind it in the middle. Another artery usually passes behind the hepatic (liver) duct and then gives off the cystic artery before entering the right lobe of the liver, but variations are common. In 75 percent of people, the cystic duct enters the common duct at an angle.
In the remainder, it runs parallel to the hepatic duct or winds around it before joining. These variations add a certain element of surprise to the routine removal of a gallbladder.
It is 11:27, and LEDs on the ventilator show the body’s pulse is 50, blood pressure 135/81. The surgeons hand the nurse bloody wads of cotton towel, which he drops in the basin of saline and the other nurse retrieves to jam in plastic disposal bags on the floor. The surgeons’ gloves are filmed with wetness. Faint wisps of pink slide across the smooth rubber. Small silver clips are pinched onto the blood vessels connected to the gallbladder. “Three-oh.” A surgeon extends a palm. Four rubber hands grasp forceps and hold them in place on the organs. One hand, fingers through the handle of silver needle drivers, deftly threads a curve of needle and silk through a pinch of glossy beigeness. Four hands take up the ends of the stitch with their needle drivers and rotate gracefully at the wrist; a knot is tied. They rotate again, the drivers bring up two ends of silk and lay them flat against the organ’s side. “Clamps back,’’ says the surgeon, extending a palm toward the nurse. He glances at the anesthesiologist. “He’s okay with you, chief?” “He’s okay.”
The junctures of gallbladder, with ducts and tendons, are clamped shut by the rubber hands. Five black silk ligatures festoon the organ. As in less gruesome sewing circles, the surgeons spend this time chatting. They discuss upcoming operations.
While forceps hold the liver out of the way, more hands grip a silver scalpel. Another pair of hands touches the yellow pencil against the scalpel to heat it. More saline solution is squirted over the organs; the suction tube pumps up a few more red beads. With short, precise strokes, the scalpel cuts at the tendon connecting the gallbladder to the backside of the liver.
Then with a swift gesture, a knit-cuffed arm plucks the gallbladder out and into a silver dish the nurse holds. The silver dish is quickly placed at the far end of a rolling metal chest, out of sight. Bloody towels are lifted out of the cavity. The forceps are taken off the organs. Together, the surgeons count aloud the forceps and scalpels in view as they are returned to the nurse's tray. They mustn’t, of course, stitch up the body with a tool left inside.
The edges of fascia are drawn together with forceps. More curves of needle and wire are slung through the mucousy tissue. Four pairs of drivers grasp long reins of stainless steel wire radiating out from the stitches. Five, six threads radiate up at each side of the seam, resembling the hoisted oars of a Viking ship.
After the gallbladder is removed, the bile ducts take over its duties. It may be three or four months before they function smoothly. During this time the patient may suffer from mild indigestion or pains caused by spasms of the common bile duct. Stones sometimes reform in the common duct after surgery. This requires another operation.
It is time to inject dye into the remaining ducts and x-ray the abdomen. This will ensure that the clips are secure. The dye process will also detect any gallstones that might be lodged in the cystic duct. The orange pancreas is now more fully visible. There are lavender touches and a deep-red line of tendon across it at an angle. A surgeon bends into the body with a syringe.
As the surgeons leave the body’s side for the x-raying, a nurse places a cotton towel over the open cavity like a gesture of modesty. The body and the table it occupies are tilted with a notching sound. A waist-high, rolling screen is placed between the table and the corner where the surgeons wait, discussing points of technique. Another screen protects the anesthesiologist, who must not leave the body.
“Three, two, one, shot.”
“Three, two, one, shot.”
It is 11:55, and the LED reads pulse 52. Blood pressure is 112/70. The x-ray machine is wheeled away, and soon more gray pictures are on the white, illuminated window. An empty space meets the ends of the cystic duct, the hepatic ducts. A tiny starburst shadow in the cystic duct indicates a gap where dye seeped through.
The surgeons take up position again. One rests a foot on the table’s rail; cowboy at a bar. He holds the cystic duct between forceps while another surgeon secures the leak with a silver clip, very quickly. A nurse takes out another paper pouch of needle and wire and opens it. He dips a bulb irrigator into the saline solution, fills it up.
Another irrigator rests in a silver, curved pan between the aqua-draped knees. Hands force the suction tube down inside the cavity. Another surgeon thrusts his hand deep inside. He grimaces. He wriggles his fist back toward himself, distending the copper-painted flesh beneath the aqua drape. His other hand finds the distention on the opposite side of the flesh, depresses it with the point of a long plastic tube, finally pierces the outside of the flesh. The tube will drain the wound, remaining in place for 24 hours. Drawing it through the hole, the surgeon slides the tube briskly back and forth: the skin edging the puncture curls inward with one stroke, then unfurls when the tubing is slid outward. There is no blood. The anesthesiologist pushes the nasogastric tube down a little at a surgeon’s instruction.
Pulse is now 66. Silver needle drivers hook another metal curve through the fascia and muscle. The pink globular fat is closing in on each side. Knot after knot of wire is twisted in careful choreography. The long ends of stainless steel are held in bunches. At 12:09, pulse is at 54, blood pressure 123/76. Three knots secure each length of wire. It takes 12, 13 stitches to pucker shut the first layer of tissue. The suction tube descends again to swallow the irrigator’s leavings.
Another layer of ligatures is braided into the fascia. Then a surgeon takes silver forceps to the stretched edges of skin and the forgotten outside of the body is reinstated again. As the tool aligns and clamps the far end of the cut together, more hands follow with a white plastic staple gun. The tender flesh is pinched and stapled quickly. It takes 19 staples to close the wound. The sides meet evenly at the end of the seam.
The surgeons move away, the tray of silver tools is rolled back. One nurse drops the gallbladder, slightly shriveled, less luminous than before, into a little jar of solution that the other nurse holds out to him. She leaves with the jar, bound for pathology, where the organ will be examined.
The anesthesiologist pulls the tape from the body’s eyes, disconnects the endotracheal tube and the esophageal stethoscope. For 15 minutes, he has been easing the patient off the mechanical ventilator and increasing the flow of sodium Pentothal and morphine through the IV. The patient is breathing on his own again: he coughs,^chin lurching upward, as the endotracheal tube is removed. The anesthesiologist’s motions are rapid. He slaps one gray cheek. “Jerry, open your eyes for me. Jerry.’’ The eyelids flutter and the man mews weakly.
Many thanks to UCSD Medical Center, Dr. A.R. Moossa, Dr. Ralph Crumb, Dr. Peter Edelstein, Dr. Doug Richardson; Joe Smith, R.N.; Maria Camilon, R.N.; Nancy Stringer; and Mr. Goss.
Here's something you might be interested in.
UCSD shows exactly what gall bladder surgery is like
Under the knife
UCSD shows exactly what gall bladder surgery is like
Under the knife
More than 20 million people in the US have gallstones in their gallbladders.
Two rubber-veiled hands press cloths down; the pumpkin square of abdomen shines taut. Framing the exposed area, faded aqua drapes conceal curves of body. Another sheathed hand grasps a silver blade, angles it with delicacy toward the skin. The blade is glided in deeply. There is no dramatic pause before that shock of knife in skin.
“Gallstones are the tombstones of infection,” goes one maxim.
For seven inches, the scalpel is drawn across the orange patch of flesh, right through. Concealed by the faded sheets, it is not a man who has been slit open, but a vessel temporarily commandeered by science. For the two hours this cholecystectomy will take, the body has no gestures, no language of its own.
The surgeons squinted at the bluish ghosts of organs on a viewing screen.
Historical medical literature, dating as far back as the days of the Talmud, reveals a knowledge of gallbladder disease and gallstones. As the human diet became more complex, cholecystitis and cholethiasis became more common. Richer, fattier foods and a sedentary lifestyle made the gallbladder function less efficiently and, consequently, more prone to form gallstones. Today, gallbladder disease and gallstones are common complaints.
A hand holding the forceps grasps a tip of the liver’s lower edge, lifting it gingerly, revealing the gallbladder, nestled against the liver’s back.
The man whose body lay pale and naked in UCSD Medical Center’s Operating Room 3 suffered from increasingly frequent attacks of pain, the result of gallstones. As in almost all cases of surgery for gallstones, the man’s entire gallbladder was to be removed. Cholecystectomy is considered a major operation but not a dangerous one. The mortality rate is less than one percent. Fatalities mostly occur in very complicated cases or in people who seek treatment too late.
It is 11:27, and LEDs on the ventilator show the body’s pulse is 50, blood pressure 135/81.
Half an hour before the first incision, the patient’s process of subjugation had already begun.
The surgery ward was slightly shabby, peeling blue paint on the doorjambs. Room 3 smelled of nothing — a sterile smell.
Five, six threads radiate up at each side of the seam, resembling the hoisted oars of a Viking ship.
One wall was covered with metal screens to ventilate the room with “relatively germ-free” air, said the scrub nurse. In the center of the roughly 15-foot-square room was the gurney and, motionless on it, the patient. His flesh was pasty in the cold light. Sparse dark brown hair on his groin, abdomen, and arms. At his head, the anesthesiologist -made adjustments on an array of machines: blood pressure, heart rate, blood oxygen level, breathing patterns are monitored. An EEG monitor to read his brain waves. At the body’s feet, a mobile steel basin on a pedestal contained a silver pitcher standing in several inches of saline solution. The silver pitcher held what looked like a meat baster — a bulb irrigator, also filled with saline. The aqua-suited surgical team talked easily as they made their routine preparations. In the presence of this man sleeping, penis exposed, their informality seemed almost callous.
The man’s grayish face was vised in tubes and tape. The tubes attached him to a mechanical ventilator animated by flashing LEDs and hissing sounds. A long line of esophageal stethoscope disappeared into his mouth at one end and into the anesthesiologist’s left ear at the other end. The patient’s eyes had been lubricated and sealed shut with surgical tape. He looked dead. At his temples, electrical clips on white adhesive disks, as if his head were a car battery to be charged. The anesthesiologist, standing behind the head, threaded a long curve of nasogastric tube into the nose, through which the stomach’s contents would exit. A probe was inserted into one of the patient’s fingertips, a pulse oximeter, to measure the oxygen level in his blood. His mouth was taped around a small plastic frame. Attached in the frame, a corrugated endotracheal tube from the ventilator brought his lungs a mixture of 43 percent oxygen and 55 percent nitrous oxide and isoflurane. The ventilator deflated his lungs again, measured via a capnograph the carbon dioxide leaving his lungs, breathed more oxygen and nitrous oxide and isoflurane into him. Through an IV in one arm, a mixture of sodium Pentothal and morphine entered his blood stream. The anesthesiologist injected him with vecuronium, a neuromuscular relaxant that would seduce his muscles into admitting the surgeon’s knife with little resistance.
A nurse unwrapped a plastic tube attached to a brown rubber coupling. She winced, then swiftly jammed it into the opening of the patient’s urethra. Seconds later, a small stream of golden urine slid slowly down the tube to a plastic bag lying on the floor. The nurse squatted down, nudged the bag under the edge of the gurney. A surgeon with a disposable razor shaved the coarse hair from the patient’s abdomen. Tearing off a wide swatch of adhesive from a roll, he daubed up the loose hairs from the shorn belly. A nurse drew up a sheet, worn soft, over the patient’s legs. As if in afterthought, she settled a white towel over the small, curled penis.
A large x-ray machine was wheeled in, and the room was cleared for the procedure. The team members stood in the hallway, talking shop. A nurse passing down the hall paused to chat with the scrub nurse: “You still here?” “Yeah.” “Whatcha doing?” “Gallbladder.” “Yeah?” “You on tonight?” "Yeah.”
Five minutes later, the surgeons squinted at the bluish ghosts of organs on a viewing screen. The gallbladder was a dwarf on the biliary tree, nearly obscured by the ovals of liver, pancreas, kidney, and adrenal gland.
In the center of the room, a nurse positioned a tray of Betadine solution and sponges on wooden sticks at the body’s side. She stroked the clammy stomach with frothy reddish-brown liquid, wiped it away again. Six times with soap, three times with Betadine, to make the skin as sterile as possible. The give of skin under the swab’s pressure briefly made the body seem tender and alive.
A length of plastic wrap, orange with Betadine, was rolled over the hairless, pale brown abdomen and pressed smooth. Faded aqua cloths were draped over the body, leaving the plastic-covered area exposed. The edges were taped and covered with gauzy white towels. The anesthesiologist raised a metal frame on either side of the neck and slipped an aqua curtain between the two poles. The body lay visually decapitated.
Gallbladder disease is generally caused by a bacterial infection, resulting in acute or chronic inflammation — like infections of the appendix, tonsils, or any other organ. If the gallbladder is inflamed, the blood supply to its walls may be restricted, and the gallbladder may fill with pus, even become gangrenous.
In some cases, though it is not known why, chronic inflammation causes gallstones. Disease can also result from a functional disturbance — the gallbladder failing to empty when it is called upon to secrete bile — or a chemical disturbance, causing stones to leave the bile and possibly obstruct its flow. A stone in the cystic duct, which runs between the gallbladder and the common bile duct, is most often the cause of inflammation.
High body temperature, pain and tenderness near the gallbladder, and an elevated white blood cell count all indicate acute inflammation. A gallbladder operation is then imperative. The pain of the inflammation is said to be dull and deep, shifting when you change position.
The cystic duct normally has the diameter of a pencil. When the gallbladder contracts during the digestive process, any stone (usually larger than the duct) would be forced into this tube. Eventually, the stone either drops back into the gallbladder and the attack subsides; remains stuck, producing acute infection requiring more or less immediate surgery, or passes on through the cystic duct into the common bile duct, possibly lodging at the juncture of the two. Should the latter take place, the entire flow of bile is obstructed, causing jaundice.
Before finally undergoing cholecystectomy, the afflicted person may contend with chronic indigestion, bloating, heartburn, nausea, flatulence, “excruciatingly knifelike” pain shooting from the upper abdomen straight up through the right shoulder, and jaundice. Cholecystatic diseases are also often accompanied by pruritus — itching — a source of severe discomfort in some cases. Pruritus usually appears about the same time as jaundice or a little before it. The itching is most severe on the extremities and is aggravated by warm, humid weather. Once thought to correspond to the levels of bile salts in the skin, the cause of the pruritus remains obscure.
If an operation is not performed, jaundice can persist, and the patient may eventually die from the toxic effects of the bile build-up. Unchecked inflammation can result in gangrene or a rupture of the organ. Either of these eventualities can cause fatal peritonitis unless immediate surgery is performed. Cancer of the gallbladder develops in approximately one to two percent of those patients who have chronic gallbladder inflammation with stones.
More than 20 million people in the US have gallstones in their gallbladders. It is estimated that approximately 25 percent of all women and 10 percent of all men will develop gallstones at some time or other before they reach 60 years of age. About 300,000 operations are performed annually for this disease, and at least 6000 deaths result from its complications or treatment. The possibility of gallbladder disease rises with age.
Cholesterol gallstones are found most often in American Indians. Frequency is lower in whites, and lowest in blacks. More than 75 percent of American Indian women over age 40 are affected. Before puberty, the disease is rare but equally frequent in both sexes. Between the ages of about 35 and 55, women are affected with three times the frequency of men. Hormonal changes caused by pregnancy, and the use of oral contraceptives, may be responsible for its greater frequency in women. After menopause, however, the disparity in gallstone incidence between men and women narrows.
The formation of gallstones is a mystery. The prevalent theory is that an upset in a patient’s chemistry — specifically, failure of fat and cholesterol metabolism — causes stones to crystallize and separate out from the fluid bile. Another theory is that stones are the aftermath of previous infection which may have occurred many years before. “Gallstones are the tombstones of infection,” goes one maxim.
Stones can vary in size from a millet seed to a hen’s egg. There is no correlation between the number and size of the stones and the symptoms they produce. Sometimes a single small stone can cause more trouble than a large one or many jagged ones.
The gallstones in 75 percent of patients are composed predominantly of cholesterol and are called cholesterol stones. The remaining 25 percent are pigment stones. Regardless of composition, the gallstones have similar consequences.
Cholesterol gallstones result when the liver secretes bile that is supersaturated with cholesterol. Influenced by unknown factors present in bile, the cholesterol separates from solution. It is thought that in the calm harbor of the gallbladder, small grains of pigment, called nidi, join the crystals, along with a mucoprotein paste. The newly formed crystals grow into stones of a size easily visible with the naked eye. They sometimes make their way out of the gallbladder in bile, lodging in the nearby ducts.
Pigment stones account for 25 percent of gallstones in the US and 60 percent of those in Japan. They are black, sometimes dark brown, 2 to 5 mm in diameter. Their frequency is similar in men and women, and in blacks and whites, but rare in American Indians. Cirrhosis, bile blockage due to a dilated common duct, and chronic hemolysis (the breaking apart of red blood corpuscles) are favorable conditions for pigment-stone formation. About 90 percent of pigment stones are composed of dense mixtures of bacteria with the pigment solids. It is speculated that bacteria could have a primary role in pigment gallstone formation, which would help to explain why people with pigment gallstones develop sepsis (toxicity caused by the absorption of bacteria into the blood stream) more often than do those with cholesterol gallstones.
The mere existence of stones doesn’t necessitate immediate surgery, but it is often suggested as a means to avoid future complications. It is believed there are many people living comfortably with gallbladders filled with stones who never develop symptoms.
In the US, only about 30 percent of people with cholelithiasis end up in surgery. Each year, about two percent of those with asymptomatic gallstones develop symptoms.
The tendency is to operate on younger patients and “temporize” in the elderly.
Little is audible above 11 the vacant whoosh of the ventilator. A high tone marks the rhythm of the patient's heart, adding a theatrical tension to the proceedings. There is no clinking of metal heard as a nurse fusses with a tray of tools overhanging the aqua-draped legs. Mumbles from behind six face masks direct the movements of twelve hands.
The white cotton cloths around the incision seep red as a surgeon’s hands push down. Under the pressure of the antiseptic plastic wrap stretched over the abdomen, the opened skin springs back, revealing a garish-pink layer of fat.
“Okay, we’re in.” A surgeon hands over his metal instrument, takes the yellow plastic pencil that a nurse hands him. A delicate silver point projects from the pencil’s tip. The other end is attached by a yellow plastic cord to a low-standing machine. A dial on the machine reads: scalpel, 35 watts. The surgeon braces one beige rubber wrist against the body’s right hipbone. He draws the yellow “hot knife” shallowly through the fat, tracing the incision. Wisps of smoke curl up, catching the light from the surgical lamps focused on the work. The odor of scorched skin rises. “Smells like barbecue, doesn’t it?” says a nurse.
As the beige hands draw the yellow pencil again and again, the cauterized fat parts. A gorge is formed. Periodically, the pencil is removed and wiped against an abrasive pad on the pencil’s yellow plastic holster, lying on the body’s shoulder. Tiny shreds of tissue cling to the abrasive surface. Another hand lowers a suction tube down, holds it against one suety wall. The walls of the gorge are formed of glossy curds, deep pink. The rubber hands descend into the ravine, stroking the fat apart. The valley widens as gauzy white cloths are firmed against the walls. The exertion raises bluish tendons up under the rubber gloves.
Another surgeon enters the room. A nurse draws gloves over his damp, upheld hands, pulls a knit-cuffed gown up his arms and cinches it at his back. The surgeon moves to the table, leans against the body’s hip to peer at the crevice of flesh and jelly. The surgeon with the hot knife backsteps, ceding his place to the newcomer. The movement is precise and elegant. Beneath the fat, a thin taut skin is now visible: the fascia, a layer of muscles and the tissues that connect them. The fascia is sheer and white; cords of pinkness cross the dark mass beneath. The surgical field is perhaps five inches wide and visible through the complete length of the incision. A nurse hands the surgeon a saline-filled bulb irrigator. Solution is squirted against the pale membrane, and the suction tube dives down to draw up a liquid the color of strawberry Kool-Aid. Beads of it hurry along the crystalline plastic suction tube toward a container next to the ventilator. The beads catch the surgical lamps’ glare, dazzling as rubies.
Very close to the open body, there is a vague warm scent, nearly overpowered by the Betadined stomach. It is the smell of sex, fertility — light and sweet and rich with blood. A surgeon lowers the electrocautery pencil between the three-inch pink walls, draws it down the fascia. As the thin tissue springs.apart, saline solution is quickly squirted in the rift, into which the suction tube swoops again to draw up in its beak. The yellow pencil is withdrawn. Another surgeon cups a curving silver spatula inside, against the wall of fat, coaxing it back.
The organs look like stones on a creek bottom. They lie with flat sides upward — the sherbet-orange surface of the pancreas tucks under a beige curve of a kidney. The liver, slightly to the left as one faces across the body, is deep mauve. The organs are smooth and glistening. Two pairs of hands push wedges of white cloth in to hold the fat layer at bay. A hand holding the forceps grasps a tip of the liver’s lower edge, lifting it gingerly, revealing the gallbladder, nestled against the liver’s back. Another pair of forceps in another hand takes hold of the gallbladder’s lower end, pulls it gently down into view. In size and shape, it resembles a pickled white pear, with a pink and blue lace just beneath its surface.
The gallbladder is a small sac, lying partially attached to the underside of the liver, in the groove between its two lobes, in the upper right portion of the abdomen. Located just beneath the arch of the ribs, it connects at its bulbous top with the liver by means of the two hepatic ducts. The sac’s narrow end connects with the top of the duodenum (the first part of small intestine) via the cystic duct, which meets the common bile duct.
This small organ’s function is to store and concentrate the bile produced and secreted by the liver. It holds about 50 ml. of bile when full. When food is eaten, particularly fatty food, the gallbladder contracts and a sphincter at the end of the common duct relaxes. During the moments when the pressure in the duct exceeds the sphincter’s resistance, bile is forced into the duodenum in squirts. The intestine will receive a supply of diluted bile directly from the liver, as well. It is essential for the digestion of fats and fatlike substances.
The gallbladder’s mucous membrane is thrown into prominent ridges when the organ is collapsed. The ridges flatten when the gallbladder is distended. Tall columns of cells form the gallbladder’s mucous membrane and are covered by hairlike microvilli on one side.
Wide channels separate the individual cells. The connecting ducts’ walls contain only small amounts of smooth muscle, except for the sphincter ringing the end of the common duct. The gallbladder musculature is made of interlocking bundles of long and spiraling fibers.
A ligament holds the internal organs in place from liver to duodenum. There is an artery to the left of the common duct and a vein, the portal vein, lying behind it in the middle. Another artery usually passes behind the hepatic (liver) duct and then gives off the cystic artery before entering the right lobe of the liver, but variations are common. In 75 percent of people, the cystic duct enters the common duct at an angle.
In the remainder, it runs parallel to the hepatic duct or winds around it before joining. These variations add a certain element of surprise to the routine removal of a gallbladder.
It is 11:27, and LEDs on the ventilator show the body’s pulse is 50, blood pressure 135/81. The surgeons hand the nurse bloody wads of cotton towel, which he drops in the basin of saline and the other nurse retrieves to jam in plastic disposal bags on the floor. The surgeons’ gloves are filmed with wetness. Faint wisps of pink slide across the smooth rubber. Small silver clips are pinched onto the blood vessels connected to the gallbladder. “Three-oh.” A surgeon extends a palm. Four rubber hands grasp forceps and hold them in place on the organs. One hand, fingers through the handle of silver needle drivers, deftly threads a curve of needle and silk through a pinch of glossy beigeness. Four hands take up the ends of the stitch with their needle drivers and rotate gracefully at the wrist; a knot is tied. They rotate again, the drivers bring up two ends of silk and lay them flat against the organ’s side. “Clamps back,’’ says the surgeon, extending a palm toward the nurse. He glances at the anesthesiologist. “He’s okay with you, chief?” “He’s okay.”
The junctures of gallbladder, with ducts and tendons, are clamped shut by the rubber hands. Five black silk ligatures festoon the organ. As in less gruesome sewing circles, the surgeons spend this time chatting. They discuss upcoming operations.
While forceps hold the liver out of the way, more hands grip a silver scalpel. Another pair of hands touches the yellow pencil against the scalpel to heat it. More saline solution is squirted over the organs; the suction tube pumps up a few more red beads. With short, precise strokes, the scalpel cuts at the tendon connecting the gallbladder to the backside of the liver.
Then with a swift gesture, a knit-cuffed arm plucks the gallbladder out and into a silver dish the nurse holds. The silver dish is quickly placed at the far end of a rolling metal chest, out of sight. Bloody towels are lifted out of the cavity. The forceps are taken off the organs. Together, the surgeons count aloud the forceps and scalpels in view as they are returned to the nurse's tray. They mustn’t, of course, stitch up the body with a tool left inside.
The edges of fascia are drawn together with forceps. More curves of needle and wire are slung through the mucousy tissue. Four pairs of drivers grasp long reins of stainless steel wire radiating out from the stitches. Five, six threads radiate up at each side of the seam, resembling the hoisted oars of a Viking ship.
After the gallbladder is removed, the bile ducts take over its duties. It may be three or four months before they function smoothly. During this time the patient may suffer from mild indigestion or pains caused by spasms of the common bile duct. Stones sometimes reform in the common duct after surgery. This requires another operation.
It is time to inject dye into the remaining ducts and x-ray the abdomen. This will ensure that the clips are secure. The dye process will also detect any gallstones that might be lodged in the cystic duct. The orange pancreas is now more fully visible. There are lavender touches and a deep-red line of tendon across it at an angle. A surgeon bends into the body with a syringe.
As the surgeons leave the body’s side for the x-raying, a nurse places a cotton towel over the open cavity like a gesture of modesty. The body and the table it occupies are tilted with a notching sound. A waist-high, rolling screen is placed between the table and the corner where the surgeons wait, discussing points of technique. Another screen protects the anesthesiologist, who must not leave the body.
“Three, two, one, shot.”
“Three, two, one, shot.”
It is 11:55, and the LED reads pulse 52. Blood pressure is 112/70. The x-ray machine is wheeled away, and soon more gray pictures are on the white, illuminated window. An empty space meets the ends of the cystic duct, the hepatic ducts. A tiny starburst shadow in the cystic duct indicates a gap where dye seeped through.
The surgeons take up position again. One rests a foot on the table’s rail; cowboy at a bar. He holds the cystic duct between forceps while another surgeon secures the leak with a silver clip, very quickly. A nurse takes out another paper pouch of needle and wire and opens it. He dips a bulb irrigator into the saline solution, fills it up.
Another irrigator rests in a silver, curved pan between the aqua-draped knees. Hands force the suction tube down inside the cavity. Another surgeon thrusts his hand deep inside. He grimaces. He wriggles his fist back toward himself, distending the copper-painted flesh beneath the aqua drape. His other hand finds the distention on the opposite side of the flesh, depresses it with the point of a long plastic tube, finally pierces the outside of the flesh. The tube will drain the wound, remaining in place for 24 hours. Drawing it through the hole, the surgeon slides the tube briskly back and forth: the skin edging the puncture curls inward with one stroke, then unfurls when the tubing is slid outward. There is no blood. The anesthesiologist pushes the nasogastric tube down a little at a surgeon’s instruction.
Pulse is now 66. Silver needle drivers hook another metal curve through the fascia and muscle. The pink globular fat is closing in on each side. Knot after knot of wire is twisted in careful choreography. The long ends of stainless steel are held in bunches. At 12:09, pulse is at 54, blood pressure 123/76. Three knots secure each length of wire. It takes 12, 13 stitches to pucker shut the first layer of tissue. The suction tube descends again to swallow the irrigator’s leavings.
Another layer of ligatures is braided into the fascia. Then a surgeon takes silver forceps to the stretched edges of skin and the forgotten outside of the body is reinstated again. As the tool aligns and clamps the far end of the cut together, more hands follow with a white plastic staple gun. The tender flesh is pinched and stapled quickly. It takes 19 staples to close the wound. The sides meet evenly at the end of the seam.
The surgeons move away, the tray of silver tools is rolled back. One nurse drops the gallbladder, slightly shriveled, less luminous than before, into a little jar of solution that the other nurse holds out to him. She leaves with the jar, bound for pathology, where the organ will be examined.
The anesthesiologist pulls the tape from the body’s eyes, disconnects the endotracheal tube and the esophageal stethoscope. For 15 minutes, he has been easing the patient off the mechanical ventilator and increasing the flow of sodium Pentothal and morphine through the IV. The patient is breathing on his own again: he coughs,^chin lurching upward, as the endotracheal tube is removed. The anesthesiologist’s motions are rapid. He slaps one gray cheek. “Jerry, open your eyes for me. Jerry.’’ The eyelids flutter and the man mews weakly.
Many thanks to UCSD Medical Center, Dr. A.R. Moossa, Dr. Ralph Crumb, Dr. Peter Edelstein, Dr. Doug Richardson; Joe Smith, R.N.; Maria Camilon, R.N.; Nancy Stringer; and Mr. Goss.
Comments